Article
LGBT Adults Are More Likely to Experience Mental Health Hardships, But Less Likely to Get Needed Help

Article
Fact-based, data-driven research and analysis to advance democratic debate on vital issues shaping people’s lives.
Center for Economic and Policy Research
1611 Connecticut Ave. NW
Suite 400
Washington, DC 20009
Tel: 202-293-5380
Fax: 202-588-1356
https://cepr.net
Belonging to the lesbian, gay, bisexual, transgender, queer, intersexual, asexual, plus other non-straight, non-cisgender (LGBTQIA+) community can be a source of strength, but also brings unique challenges that can have a negative impact on mental health. These challenges include discrimination and stigmatization based on gender identity and sexual orientation.
To inform policy and other discussions around LGBTQIA+ mental health, this article uses the Census Bureau’s Household Pulse Survey (HPS) to document mental health disparities by gender identity and sexual orientation. Consistent with prior research, it documents that LGBT adults are more likely to report experiencing mental health hardships than non-LGBT respondents (the analysis is limited to LGBT adults because the HPS does not include sufficient questions to cover the full range of LGBTQIA+ identities). Yet at the same time, LGBT respondents were less likely to get the counseling and therapy they needed.
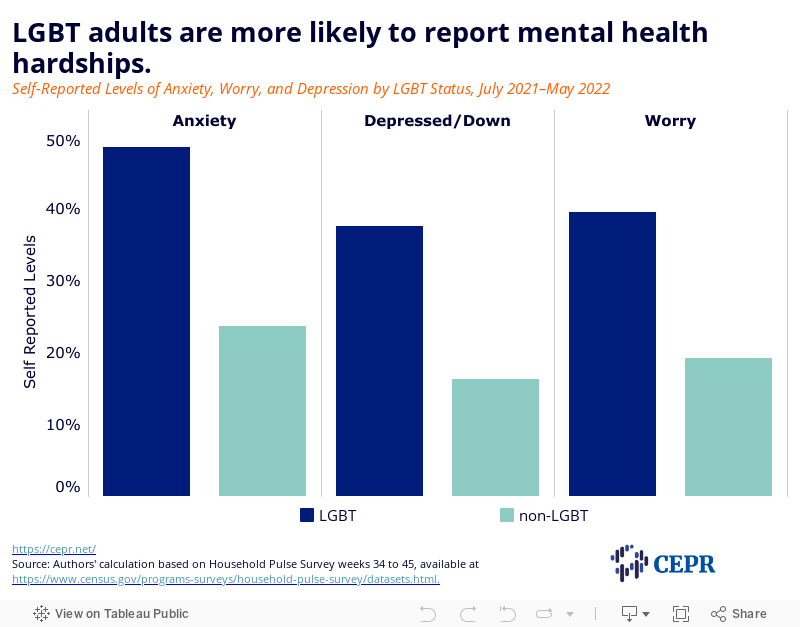
About one in two LGBT adults (48 percent) reported feelings of anxiety for more than half the days in the two weeks prior to responding to the survey, compared to less than one-quarter (23.5 percent) of non-LGBT adults.
Nearly four in 10 LGBT adults (39 percent) reported feelings of uncontrollable worry for more than half the days in the two weeks prior to responding to the survey, compared to less than one-fifth (19 percent) of non-LGBT adults.
More than one in three LGBT adults (37 percent) reported feelings of depression or hopelessness for more than half the days in the two weeks prior to responding to the survey, compared to only one-sixth (16 percent) of non-LGBT adults.
Younger LGBT adults (18–34) were more likely to report mental health hardships than older LGBT adults (35–64). There was a similar disparity between younger and older non-LGBT adults. However, older LGBT adults were still more likely to report mental health hardships than younger non-LGBT adults.
More than one in three LGBT adults (36 percent) reported using prescription medication for mental health-related disorders, compared to only one-fifth (21 percent) of non-LGBT adults.
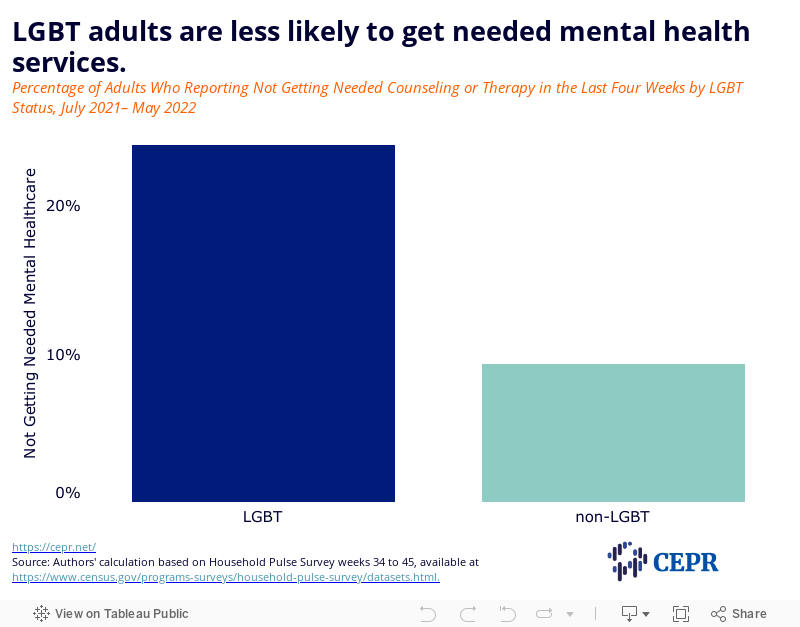
Nearly one in four LGBT adults (24 percent) reported not being able to access mental health services when they needed them, compared to less than one-tenth (9 percent) of non-LGBT adults.
All people should have the right to comprehensive and accessible mental health care. The best way to provide such a guarantee would be through a single-payer system like Medicare for All. Eliminating mental health disparities between LGBTQIA+ and non-LGBTQIA+ people willl also require fundamental reforms that end discrimination on the basis of sexual orientation and gender idenitity.
The HPS asks adult respondents, in the two weeks prior to taking the survey, how often they have been bothered by: 1) feeling anxious, on edge, or nervous; 2) not being able to stop worrying; and 3) feeling down, depressed, or hopeless. In the figures below, adults are classified as having a mental health hardship if they report having one of these feelings (anxiety, worry, or depression) for at least half the days in the applicable look-back period.
As Figure 1 shows, nearly half of LGBT adults reported experiencing anxiety, and just under 40 percent reported worry or depression. Compared to non-LGBT adults, LGBT adults were at least 20 percentage points more likely to report experiencing each of the three hardships.
Figure 1
The HPS also asks respondents whether: 1) they have taken prescription medication to help with emotions, concentration, behavior, or mental help in the last four weeks; and 2) they needed counseling or therapy from a mental health professional in the last four weeks, but did not get it.
Figure 2 shows that about one in three LGBT adults has taken prescription medication for a mental health-related reason, compared to just over one in five non-LGBT adults. At the same time, as Figure 3 shows, nearly one in four LGBT adults reported needing counseling or therapy that they did not receive, as did nearly one in ten non-LGBT adults.
Figure 2
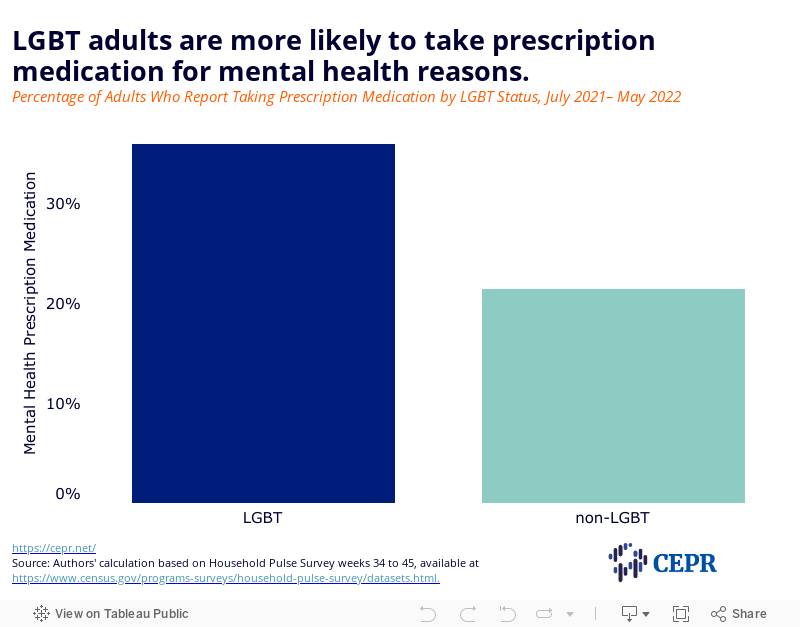
Figure 3
In the HPS and other surveys, younger respondents are much more likely to self-identify as LGBT than older ones. In the sample from HPS used in this analysis, nearly 34 percent of LGBT adults are between 18 and 34, compared to only 12 percent of non-LGBT adults. This raises the question to what extent mental health disparities by LGBT status are due to differences in the age composition of LGBT and non-LGBT adults.
To provide an initial look at this question, Figures 4 and 5 categorize non-elderly adults by age as younger (18–34) or older (35–64). Figure 4 shows that younger LGBT adults are more likely to report mental health hardships than older ones. There is a similar, if somewhat less pronounced age divide among non-LGBT adults. At the same time, older LGBT adults are still more likely than younger non-LGBT adults to experience each of the three mental health hardships.
Figure 4
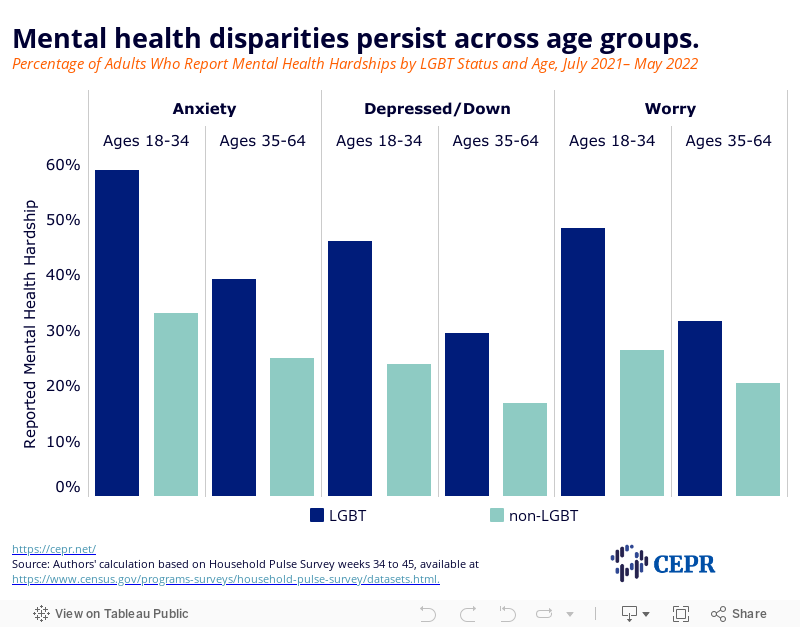
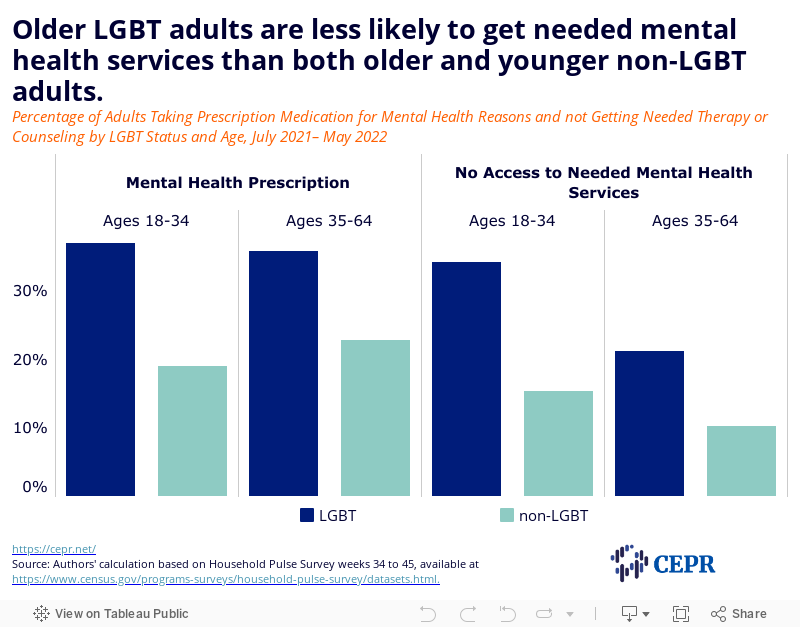
Figure 5 shows age differences in not getting needed counseling or therapy, and taking prescription drugs for mental health reasons. The age divide in not getting needed counseling or therapy is similar for both LBGT and non-LGBT adults. Here again, older LGBT adults are more likely to report not getting needed counseling or therapy than both younger and older non-LGBT adults. When it comes to taking prescription medication for mental health reasons, there is little difference between younger and older LGBT adults. However, younger non-LGBT adults are less likely to take prescription medication than older ones.
Figure 5
In a recent report, the US Department of Health and Human Services (HHS) found that 12.7 percent of LGB+ adults were uninsured in 2019. (The report used the National Health Interview Survey, which has sexual orientation questions, but no gender identity ones.) Despite there being no significant difference in uninsurance rates of LGB+ and non-LGB+ adults, HHS found that LGB+ adults were much more likely to report delaying counseling or therapy due to costs (18.4 percent vs. 4 percent respectively) and were more worried about being able to pay a medical bill if they got sick or injured.
All people should have the right to comprehensive and accessible mental health care. While the Congress will not pass Medicare for All (M4A) this year, it should, at the very least, adopt drug pricing reforms, permanently extend temporary improvements to the Affordable Care Act that reduce the cost of coverage in the ACA Marketplace, and close the coverage gap for low-income people who live in holdout states that have refused to expand Medicaid. Both reforms would increase access to, and reduce the cost of, mental health services and prescription drugs for a substantial number of LGBT+ people. It is also worth noting that the Bipartisan Safer Communities Act, signed into law by President Biden last month, includes $9.6 billion to build out certified community behavioral health clinics in every state.
Eliminating mental health disparities between LGBT and non-LGBT people willl also require fundamental reforms that end discrimination on the basis of sexual orientation and gender idenitity both inside and outside the health care system.
There is little question that negative beliefs about LGBTQIA+ people, and negative actions taken on the basis of these beliefs — including by institutions, employers, family members, public figures, and others — affect mental and physical health. Negative beliefs and attitudes can be especially harmful to teens and young adults. The Trevor Project’s 2022 National Survey on LGBTQ Youth Mental Health found that LGBTQ youth (13–24) who reported high social support from their family where half as likely to attempt suicide as those who did not. Affirmative school environments, and living in a supportive community, were also related with lower suicide rates. The survey also found upticks in anxiety, depression, and considering suicide over the last few years.
According to HHS, half of treatment facilities in the United States do not offer specialized services for LGBTQ+ patients. A 2017 survey conducted for the Center on American Progress (CAP) found that 8 percent of LGBQ patients were refused service by a medical professional on the basis of their sexual identity. Transgender patients were especially likely to experience discrimination – nearly 30 percent reported being refused service based on their gender identity. A separate CAP survey conducted in 2020 found that LGBTQ people of color were much more than white LGBTQ people to experience discrimination in heath care settings.
Last year, HHS announced that its Office for Civil Rights would enforce existing laws prohibiting discrimination based on sex to include: (1) discrimination on the basis of sexual orientation; and (2) discrimination on the basis of gender identity. Despite this, and progress in some other areas, some 25 states still criminalize the transmission of, or perceived exposure to, HIV. The dangers of such laws include, but are not limited to, the perpetuation of racialized antigay stigma and criminalizing behavior unrelated to the spread of HIV, and are likely to undermine other efforts to prevent HIV transmission. The rights of transgender individuals have been increasing targeted by policymakers on all fronts. Medical coverage is at the forefront of these attacks. Fourteen states currently have transgender exclusions in state Medicaid coverage.
The mental health hardships and disparities experienced by LGBT adults have multiple causes, including discrimination (both inside and outside of the health care system), stigma, uninsurance, and inability to afford care even if insured. Fundamental changes to laws and attitudes will be needed to address the mental health hardships faced by both LGBT and non-LGBT people, and to reduce the disparities that exist between them.
Note the use of LGBTQIA+ acronyms varies throughout the article. “LGBTQIA+” is used when referring to the entire community and “LGBT” is used for the HPS data. Any other use is specific to the survey or article that is being referred to in text.
This article uses pooled Household Pulse Survey data collected by the Census Bureau on a roughly semimonthly (twice a month) basis starting July 21, 2021 and ending May 9, 2022. Adult respondents are assigned to one of the following three categories according to the Census Bureau’s methodology:
“LGBT” includes individuals who: report sexual identity as gay, lesbian, or bisexual; identify as transgender; or report their current sex as something other than their sex at birth.
“Non-LGBT” includes individuals who report sexual identity as straight, and whose current sex aligns with their sex at birth.
“Other” includes respondents who select “none of these” for current gender identity and “something else/I don’t know” for the sexual orientation question; or respondents who select “something else/I don’t know” for the sexual orientation question, and whose current sex aligns with their sex at birth.
Results for the “other” category are not reported in this article.
Consistent with the recommendations of the Center for American Progress, all observations in which the Census imputes the gender identity of a survey respondent are dropped. This is done to ensure the accurate identification of transgender individuals.
All measures are weighted using the provided person-level weights. The final sample, after dropping missing observations, consists of 46,102 LGBT and 563,329 non-LGBT individuals. This includes 15,620 LGBT and 68,876 non-LGBT adults who are 18 to 34 years old, and 24,481 LGBT and 326,827 non-LGBT adults who are 35 to 64 years old.
The HPS is an experimental data product designed by the Census Bureau to provide near real-time data on how the pandemic has affected health, well-being, and other aspects of people’s lives. The HPS is sent to about 1 million households every week, and has a very low response rate (generally less than 6 percent) compared to most other federal surveys. The Census instructs users to exercise caution when using responses to the HPS sexual orientation and gender identity questions as standalone markers of the prevalence of LGBT adults in the general population.
Treating sexual orientation and gender identity minorities as a single category for analysis (LGBT), as this article does, likely obscures important differences between distinct groups in mental health hardships and access to care. Future research on mental health using the HPS should include findings that are disaggregated by LGBT category.