May 15, 2023


The U.S. is one of only six countries worldwide that does not mandate some form of paid leave.1 Paid family and medical leave (hereafter referred to as paid leave) is a critical benefit that typically guarantees eligible workers up to 12 weeks of paid leave for personal and familial care obligations. In the absence of a federal mandate, access to paid family and medical leave depends on whether your employer voluntarily provides it, or if you live in one of the 11 states that have passed a guarantee.2
In practice, the patchwork of employer-provided and state-mandated paid leave policies covers a small subset of the U.S. workforce. In 2022, less than 25 percent of workers had access to paid family leave benefits. Access skews towards white workers, professionals, and those who work full-time.3 Without access to paid leave, many are forced to reduce their hours of employment or take unpaid leave, both of which result in lower take-home pay. In some cases, the lack of paid leave may cause an exit from the labor force when employment and care obligations conflict, particularly for part-time workers juggling the two demands. Unpacking how many people are working part-time due to care responsibilities and without access to paid leave is fundamental to understanding how the development of federal public policy, such as paid leave, may increase economic security for these workers, many of whom are poorly compensated.
In this brief, we pool together two years of monthly Current Population Survey (CPS) data4 from 2021 through 2022 to amass an adequate sample of part-time workers. The CPS defines part-time work as working less than 35 hours per week on all jobs.5 We then define a subsample of care-related part-time workers as those who worked part-time for one of the following reasons: 1) personal or family member’s serious health issue or illness, 2) childcare issue, or 3) other family obligations.
Analysis of other data sets, like the Leave and Job Flexibilities Modules of the American Time Use Survey, may be useful in addressing these limitations but is beyond the scope of this initial brief.6 However, we do briefly summarize employer-provided data on paid family leave benefits from the National Compensation Survey (NCS). This data does not include demographic characteristics, but does include some job characteristics, and clearly establishes the disparities in employer-provided leave by full-time/part-time status and wage levels.
Because women are more likely to provide care7, we focus on occupation groups where women are disproportionately represented (including healthcare support, other care support such as teaching aides and child care workers, and food service and preparation). We then predict the likelihood of care-related part-time employment by occupation, gender, and race/ethnicity (irrespective of whether part-time work is by choice or by unhappy necessity). Given the aforementioned limitation of the CPS, we draw on the NCS to discuss our findings in the context of the wide disparities in worker access to paid family and medical leave. Our conclusion is that a federal paid family and medical leave guarantee is necessary to improve the economic security of part-time workers, and would be especially beneficial to those working part-time due to care demands.
The way economic and social phenomena are defined, collected, and processed in statistical surveys—what sociologist Daniel Hirschman calls knowledge infrastructures—impacts public and expert understanding of issues like part-time work, and how much freedom people have to choose various employment arrangements.8 According to the Bureau of Labor Statistics (BLS), people work part-time for either economic or non-economic reasons, also typically referred to by economists as involuntary or voluntary part-time employment respectively. BLS classifies workers as part-time for economic reasons if they say they are able to work full-time but cannot do so because of slack or unfavorable business conditions, seasonal declines in demand, or inability to find full-time work.9 All other part-time workers are classified as voluntary, even if their reason is dealing with a serious illness, health condition, or childcare issues.
This obscures the role of public policy in structuring employment decisions. The lack of public care infrastructure and work-family policies in the U.S. directly constrain employment choices in ways that are often involuntary and fundamentally economic. Many U.S. workers have no meaningful choice but to work part-time given their own health and care obligations, and the existing, often very limited, state of employment-based and social insurance benefits related to these obligations. At the same time, some people have no choice but to work full-time, even if they would prefer to work less than full-time and spend more time providing care or caring for themselves. In both cases, characterizing these employment states as non-economic and always voluntary ignores the constraints and structures that limit workers’ ability to freely choose whether to work full-time or part-time and how much time to devote to care and family.
Prior research finds that certain groups of workers are more likely to work part-time than others; these groups include women, disabled workers, parents, and those with less than a college degree.10 Relative to full-time workers, those working part-time have much less access to benefits like paid family and medical leave; thus, examining what percentage of part-time workers work less than full-time because of care obligations is critical to understanding how policies like paid leave can increase economic security among part-time workers.
In the next section, we present descriptive and inferential analyses on the prevalence of care-related part-time employment. To inform public policy that may potentially relieve the double care duties workers encounter within and outside of the workplace, we focus our analysis on female-dominated care occupations and food service occupations to investigate if workers in those occupations are more likely to work part-time because of care obligations than workers in other occupations.
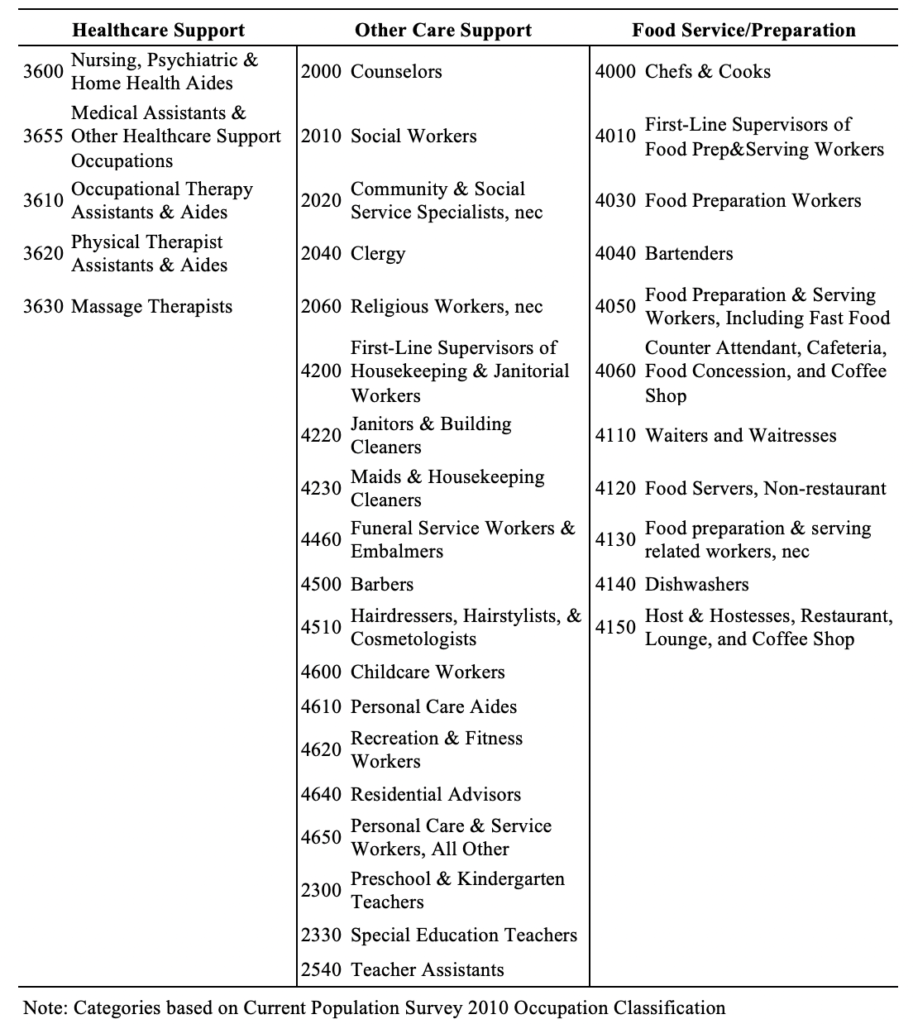
What percentage of part-time workers work part-time because of care obligations? Table 1 displays the percentage of part-time workers who are part-time because of a personal or familial health issue or child care issues by three major occupation categories including 1) healthcare support, 2) other low-wage care work such as teaching aides and child care workers, and 3) food service and preparation workers. A full list of occupations included in each category can be found in Appendix Table A2. We include all other occupations as a comparison group, and report prevalence among workers in the sample across all occupations.
Table 1
Just under one-third (31 percent) of part-time workers report working part-time because of care obligations, totaling roughly 8 million. More people work part-time because of a personal or family member’s health issue or disability (27 percent) than because of child care issues (4 percent).
Part-time workers in the three specific occupational groups we look at are more likely to work part-time for self-care or family-care reasons than part-time workers in the other occupations. Just under 40 percent of part-time workers in healthcare and other care support occupations work part-time due to care obligations. One-in-three part-time workers in food service occupations work part-time because of care obligations.
The overrepresentation of care-related part-time workers in these occupations highlights the reality that both paid care workers and low-wage service workers, who are predominantly women, are also providing significant amounts of unpaid care for themselves and their loved ones. Universal paid leave policies, which help to ensure that workers can better balance care obligations with paid employment, are critical to ensuring that those who provide care are well-cared for themselves.
Figure 1
Figure 1 displays the predicted probability of care-related part-time employment by gender, race/ethnicity, and occupation. We control for worker demographic characteristics, industry, and state of residence. Women who work part-time have a higher likelihood of doing so because of care obligations compared to men who work part-time (36 percent and 22 percent respectively). Gender disparities in care-related part-time employment reflect persistent gender inequalities in the labor market, which, among many things, are impacted by gendered divisions of paid and unpaid labor.11
After controlling for workers’ socioeconomic characteristics, women of all races and ethnicities have higher chances of working part-time because of care obligations than men. Notably, Black, Hispanic and AAPI women in healthcare support jobs are more likely to work part-time for care reasons than their counterparts in non-care occupations, as are men in all four racial/ethnic groups. Interestingly, after adjusting for their socioeconomic characteristics, part-time food service workers are no more likely to work part-time for care reasons than other part-time workers in non-care and non-food-service occupations.
Despite a large body of research on the social, economic, and health benefits of paid family and medical leave12, the ability to actually take paid leave remains out of reach for a majority of Americans. Research on the impact of paid leave guarantees in California, New Jersey, and New York finds that these leaves increase the likelihood that someone remains employed following a loved one’s health shock or disability, particularly for women.13 These findings are echoed by research which finds that, among service workers, the ability to take paid leave effectively eliminates negative health and economic outcomes from a health shock or medical condition.14
By far, our analyses reveal that net of other characteristics, women are significantly more likely to work part-time because of care obligations compared to men. Workers in low-wage occupations, such as health care aides and food services, are also more likely to work part-time due to caregiving duties than the national average. Part-time and low-wage workers generally lack access to employer-provided paid leave. This may be detrimental to their economic security whether the part-time work is due to workers’ preferences or because they have no choice.
As noted earlier, the Current Population Survey does not ask respondents about whether or not they have access to paid leave, so we are unable to directly test the relationship between access to paid leave and the likelihood of care-related part-time employment. Instead, we discuss general trends in access to employer-provided paid leave using data from the Bureau of Labor Statistics National Compensation Survey (NCS). The NCS includes employer-reported data on employees’ access to paid family and medical leave through their job. It does not include those who are covered by a state insurance program.
Figure 2 displays access to paid family and medical leave among private sector workers in 2022 by full/part-time employment status and wage quartile. In 2022, only 25 percent of civilian workers in the United States had access to paid family leave through their employers. Access to employer-provided paid leave is stratified by employment status and wage quartile. Just 12 percent of part-time workers in the U.S. had access to employer-provided paid leave in 2022, compared to 28 percent of full-time workers. Part-time workers are significantly less likely to receive employment benefits such as healthcare, retirement contributions, and work-family support policies like paid leave. High-wage workers are more likely to have access to paid leave than low-wage workers (40 percent of workers in the highest wage quartile have access to paid leave compared to just 12 percent in the lowest wage quartile). Given that 11 states have passed paid-leave guarantees, total rates of access to paid leave (both via employer and state) are likely higher.
Figure 2
Without a collective insurance pool like those created by state-level paid leave guarantees, employers must shoulder the entirety of costs associated with offering paid leave. As a result, it is unlikely that most employers will offer this critical benefit to part-time workers or those in low-wage occupations. A federal paid leave guarantee can increase the number of people who are able to take paid leave by collectivizing costs among the entire population. For the 31 percent of care-related part-time workers, a federal paid leave guarantee could increase economic security, and in some cases allow people who would otherwise not be able to look for full-time employment to do so.
About 8 million workers — 31 percent of all part-time workers— report working part-time because of care obligations. More workers are at work part-time because of a personal or family member’s health issue/disability (27 percent) than because of childcare issues (4 percent). Care-related part-time employment is particularly prevalent for women (regardless of race and ethnicity) in low-wage health care and food service occupations, where nearly two out of five workers are part-time because of care obligations.
According to the NCS, only one out of four U.S. workers had access to paid family leave through their employers in 2022. Earlier research has shown that Black and Hispanic workers, low-wage workers, and part-time workers are among the least likely to have access to paid family and medical leave.15 Policies like a federal paid leave guarantee could close these gaps, and ensure that all workers have the time and resources needed to care for themselves and their loved ones.
While this analysis primarily focuses on part-time workers, it is worth noting that some low-wage workers employed full-time (but with caregiving duties) cannot afford to work part-time because doing so would mean taking a pay cut when their employers do not provide paid leave benefits.
Taken together, these points highlight the importance of guaranteed paid leave policies as a tool for reducing occupational, ethnic, and racial disparities in access to paid leave, as well as disparities in workers’ ability to work the number of hours they truly prefer (whether full-time or part-time). These disparities require federal policy solutions, such as the Family and Medical Insurance Leave (FAMILY) Act, that ensure leave coverage and benefit levels to level the playing field for workers with care obligations. Family policies like paid leave ensure that all people have the time and resources needed to care for themselves and their loved ones. Guaranteeing the right to paid leave is a critical step in ending economic penalties for caregiving and creating a more equitable labor market for all.
The authors thank Eileen Appelbaum and Sylvia Allegretto for their valuable comments and guidance.
![]()
Table A2. Occupation Categories